
Explore the role of genetics in skin cancer risk and learn how specific mutations influence your vulnerability. Take charge of your skin health!

Genetics directly shapes your skin cancer risk through inherited and acquired DNA mutations that alter how your cells grow, repair damage, and respond to environmental threats. Genes like CDKN2A, CHEK2, ATM, and MITF p.E318K are among the most studied contributors to hereditary melanoma, while syndromes like xeroderma pigmentosum and Gorlin syndrome create extreme susceptibility in affected families. Understanding the role of genetics in skin cancer does not mean your fate is sealed. It means you have specific, actionable information to work with. This article breaks down which mutations matter, how your genes interact with UV exposure, and what you can do about it.
Which genes are most linked to hereditary skin cancer risk?
The genetic predisposition to skin cancer centers on mutations in genes that control DNA repair, cell cycle regulation, and tumor suppression. When these genes carry pathogenic variants, the body’s ability to catch and correct cellular errors weakens, and cancer becomes more likely over time.
CDKN2A is the most well-known high-risk melanoma gene. It encodes two proteins that regulate the cell cycle, and when mutated, cells can divide unchecked. CHEK2 and ATM are DNA repair genes; when either carries a pathogenic variant, the body struggles to fix UV-induced DNA breaks before they become permanent mutations. The MITF p.E318K variant is less common but specifically elevates melanoma risk, particularly in individuals with multiple primary tumors.
The numbers are telling. Pathogenic germline variants appear in 10.7% of mucosal melanoma patients, with CHEK2 and ATM being the most frequent. That figure is striking because mucosal melanoma is considered a rarer subtype with less obvious UV involvement, which confirms that hereditary factors operate independently of sun exposure in some cases. In higher-risk groups such as young patients or those with multiple tumors, familial melanoma gene variants appear in 3.2% to 7.0% of individuals, compared to less than 1% in the general population.
Beyond individual gene mutations, several hereditary syndromes dramatically increase skin cancer risk:
- Xeroderma pigmentosum: Caused by defects in nucleotide excision repair genes, this condition leaves patients unable to fix UV-induced DNA damage, resulting in a skin cancer risk hundreds of times higher than average.
- Gorlin syndrome (basal cell nevus syndrome): Driven by mutations in the PTCH1 gene, this syndrome causes multiple basal cell carcinomas to develop, often beginning in early adulthood.
- Familial atypical multiple mole melanoma (FAMMM) syndrome: Linked to CDKN2A mutations, this syndrome is characterized by numerous atypical moles and a significantly elevated lifetime melanoma risk.
Inherited defects in DNA repair and tumor suppressor pathways define these syndromes and explain why skin cancer clusters in certain families across generations. Knowing your family history is not just useful context. It is a clinical data point that can change your screening schedule.
How do genetics and UV exposure interact to cause skin cancer?
Genetics sets the stage, but environment writes much of the script. The concept of the exposome captures the full range of environmental exposures a person accumulates over a lifetime, and UV radiation sits at the top of that list for skin cancer. What makes this interaction particularly important is that it does not operate only through direct DNA mutations. It also works through epigenetics.
Epigenetics refers to changes in how genes are expressed without altering the underlying DNA sequence. UV radiation and other exposures reprogram the epigenome through mechanisms like DNA methylation and histone modification, effectively switching cancer-promoting genes on and protective genes off. A person with a CDKN2A mutation who accumulates decades of UV exposure is not just dealing with one risk factor. They are experiencing a compounding effect where genetic vulnerability and environmental reprogramming reinforce each other.
The molecular detail matters here. UV-induced photodamage disrupts mitochondrial homeostasis and increases reactive oxygen species, which accelerates cellular damage and impairs the antioxidant signaling pathways that would normally protect skin cells. This is why two people with the same CDKN2A mutation can have very different outcomes depending on their lifetime sun exposure.
Epigenetic changes serve as the critical interface between your inherited genetic susceptibility and the cumulative environmental exposures you accumulate over decades. They are not fixed at birth, which means lifestyle choices genuinely alter your cancer trajectory.
Pro Tip: If you carry a known skin cancer gene variant, applying broad-spectrum SPF 30 or higher daily and wearing UPF-rated clothing is not optional sun care. It is a direct intervention against the environmental trigger most likely to activate your genetic risk.
The practical implication is significant. Even individuals with strong genetic predispositions can meaningfully reduce their risk through consistent sun protection. Genetics loads the gun, but cumulative UV exposure often pulls the trigger.
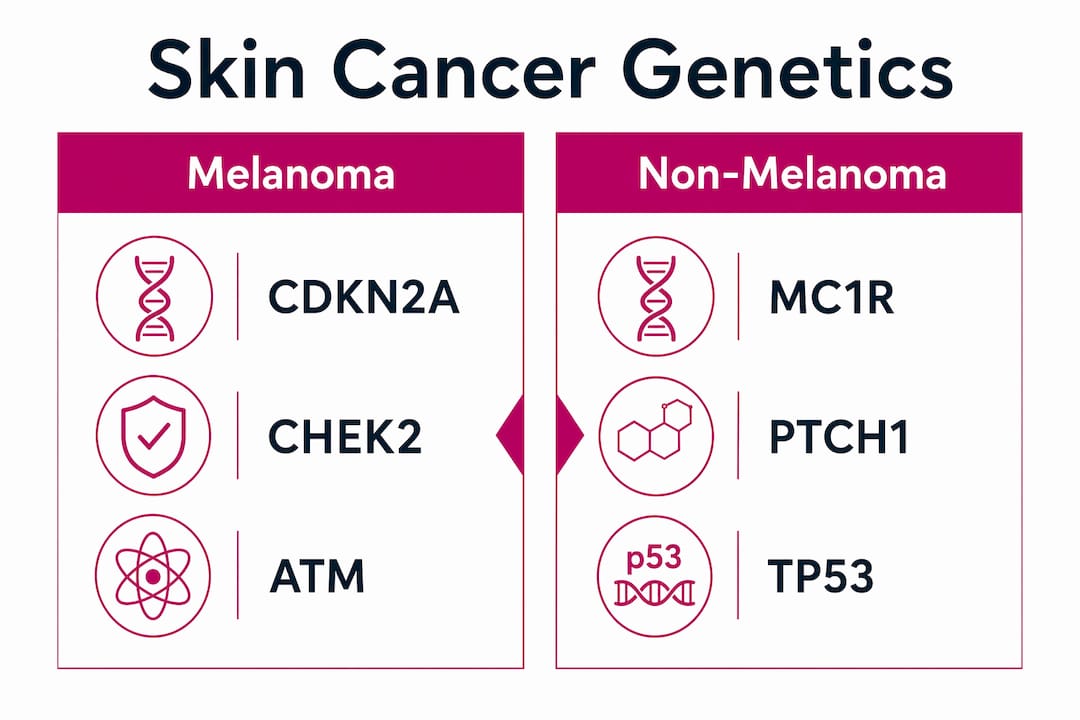
How does genetic risk differ between melanoma and non-melanoma skin cancers?
Not all skin cancers share the same genetic blueprint. Melanoma, basal cell carcinoma (BCC), and squamous cell carcinoma (SCC) each have distinct mutation profiles, and understanding those differences shapes how you screen, treat, and monitor each type. You can explore the types of skin cancer and their individual risk profiles to see how these distinctions play out clinically.
Melanoma carries the most studied hereditary component, driven by CDKN2A, CHEK2, ATM, and MITF. But melanoma also accumulates acquired mutations during a person’s lifetime. BRAF mutations appear in 40 to 60% of metastatic melanomas, and identifying this mutation transformed treatment. BRAF inhibitors and immunotherapy combinations now offer survival outcomes that were unimaginable two decades ago. This is a case where understanding the acquired genetic landscape of a tumor directly determines which treatment a patient receives.
BCC and SCC have their own genetic signatures. The MC1R gene, which controls skin pigmentation, is strongly associated with BCC risk in fair-skinned individuals. TP53 mutations are common in SCC and reflect accumulated UV damage to the genome over time. Gorlin syndrome, driven by PTCH1 mutations, creates a hereditary predisposition specifically to BCC.
| Skin cancer type | Key hereditary genes | Common acquired mutations | Hereditary syndrome |
|---|---|---|---|
| Melanoma | CDKN2A, CHEK2, ATM, MITF | BRAF (40–60% of cases) | FAMMM syndrome |
| Basal cell carcinoma | PTCH1, MC1R | PTCH1 somatic mutations | Gorlin syndrome |
| Squamous cell carcinoma | TP53 pathway genes | TP53 (UV signature) | Xeroderma pigmentosum |
| Mucosal melanoma | CHEK2, ATM | KIT mutations | No defined syndrome |
The distinction between inherited and acquired mutations also matters for prognosis. Inherited mutations define your baseline risk before any cancer develops. Acquired mutations accumulate in tumor cells and determine how aggressive a cancer behaves and which therapies will work against it. Both layers of genetic information are now used in clinical decision-making at leading dermatology and oncology centers.
What prevention strategies make sense if you have genetic risk factors?
Knowing your genetic risk is only useful if it changes what you do. The good news is that several practical strategies directly address the elevated risk that comes with a genetic predisposition to skin cancer.
- Schedule regular full-body skin exams. Individuals with a family history of melanoma or a known gene mutation should have professional skin cancer screenings at least annually, and more frequently if their dermatologist recommends it. Early detection remains the single most effective way to improve outcomes.
- Consider genetic testing. If you have a first-degree relative with melanoma or multiple family members with skin cancer, genetic counseling and testing for CDKN2A, CHEK2, and ATM variants can clarify your personal risk. Polygenic risk scores, developed by companies like 23andMe, combine multiple genetic variants with phenotype data like mole count and pigmentation to generate a more complete picture of susceptibility.
- Protect against UV exposure consistently. Broad-spectrum sunscreen, protective clothing, and avoiding peak sun hours between 10 a.m. and 4 p.m. reduce the environmental trigger most likely to interact with your genetic vulnerability.
- Monitor for new or changing lesions. Monthly self-exams using the ABCDE criteria (asymmetry, border, color, diameter, evolution) catch changes early. Photograph suspicious spots and track them over time.
- Ask about circulating tumor DNA monitoring if you have a history of melanoma. Blood-based ctDNA testing is an emerging clinical tool that detects melanoma progression and treatment resistance without invasive biopsies, giving oncologists real-time data on how a patient is responding.
Pro Tip: Genetic markers alone do not diagnose skin cancer. A complete risk picture combines your genetic results with mole count, skin tone, sun exposure history, and family history. Bring all of this information to your dermatologist appointment, not just a genetic test result.
Personalized prevention is where dermatology is heading. The days of one-size-fits-all sun safety advice are giving way to risk-stratified screening schedules and targeted monitoring based on individual genetic profiles. Understanding your skin cancer risk factors in full is the foundation of that approach.
Key takeaways
Genetics significantly shapes skin cancer risk through inherited mutations in genes like CDKN2A, CHEK2, and ATM, but cumulative UV exposure and epigenetic changes determine whether that risk becomes disease.
| Point | Details |
|---|---|
| Key hereditary genes | CDKN2A, CHEK2, ATM, and MITF p.E318K are the primary drivers of hereditary melanoma risk. |
| Epigenetics amplifies risk | UV exposure reprograms gene expression through DNA methylation, compounding inherited vulnerability. |
| BRAF changes treatment | BRAF mutations in 40–60% of metastatic melanomas enable targeted therapies that improve survival. |
| Genetic testing adds precision | Polygenic risk scores combine gene variants with phenotype data for a more accurate risk estimate. |
| Prevention remains effective | Consistent sun protection and annual screenings reduce risk even in individuals with genetic predispositions. |
What I’ve learned from watching genetics reshape skin cancer care
I have watched the conversation around hereditary skin cancer risk shift dramatically over the past decade. When patients used to mention a family history of melanoma, the clinical response was often limited to “come in more often for checks.” Now, that same family history can trigger a conversation about CDKN2A testing, polygenic risk scores, and personalized screening intervals. That shift is real progress.
But I want to be honest about something that gets glossed over in most genetic risk discussions. A positive result on a skin cancer gene panel does not mean you will get cancer. It means your baseline probability is higher than average, and that probability is still heavily shaped by what you do every day. The patients I find most at risk are not necessarily those with the most significant mutations. They are the ones who know their genetic status and then do nothing differently.
The other thing worth saying plainly: genetic testing is not yet a routine part of dermatology care for most patients. It is most valuable for people with a strong family history, multiple primary tumors, or early-onset disease. Pushing everyone toward genetic panels creates anxiety without proportionate benefit. The right approach is a conversation with a dermatologist who can assess your full picture, not a direct-to-consumer test result interpreted in isolation.
The future of personalized skin cancer prevention will combine genetic data, epigenetic markers, and real-time monitoring tools like ctDNA into a genuinely individualized risk profile. We are not fully there yet, but the trajectory is clear. For now, the most powerful thing you can do is show up for your annual skin exam, protect yourself from UV exposure, and tell your dermatologist everything about your family history.
— Krunal
How Raodermatology supports patients with genetic skin cancer risk
Raodermatology, founded by Dr. Babar K. Rao with over 25 years of experience across California, New Jersey, and New York, offers personalized skin cancer care built around your individual risk profile. Whether you carry a known genetic mutation, have a strong family history of melanoma, or simply want a thorough baseline evaluation, the practice provides skin cancer prevention, detection, and treatment services designed to catch problems early and keep you protected. From full-body skin exams to advanced treatment options for diagnosed cancers, Raodermatology’s clinical team brings the depth of expertise that genetic risk requires. Schedule a consultation to get a risk assessment that goes beyond generic advice.
FAQ
What is the role of genetics in skin cancer?
Genetics influences skin cancer risk through inherited mutations in genes like CDKN2A, CHEK2, and ATM that impair DNA repair and cell cycle control. These mutations increase susceptibility, particularly when combined with UV exposure and other environmental factors.
Does skin cancer family history mean I will develop it too?
A family history of skin cancer raises your statistical risk but does not guarantee you will develop the disease. Consistent sun protection, regular screenings, and genetic counseling can significantly reduce your personal risk even with a hereditary predisposition.
What does genetic testing for skin cancer actually tell you?
Genetic testing identifies pathogenic variants in high-risk genes and, through polygenic risk scores, estimates your overall susceptibility by combining multiple genetic markers with factors like mole count and skin tone. It informs screening frequency and prevention strategies rather than providing a definitive diagnosis.
Are melanoma and basal cell carcinoma driven by the same genes?
No. Melanoma is primarily associated with CDKN2A, CHEK2, ATM, and acquired BRAF mutations, while basal cell carcinoma is linked to PTCH1 and MC1R variants. Each type has a distinct genetic profile that shapes both risk and treatment options.
What is circulating tumor DNA and why does it matter for skin cancer?
Circulating tumor DNA (ctDNA) is genetic material shed by cancer cells into the bloodstream, detectable through a blood draw. For melanoma patients, ctDNA testing monitors treatment response and detects recurrence in real time without requiring surgical biopsies.
Recommended
- Know your skin cancer risk factors and stay protected | Rao Dermatology
- Types of skin cancer: Risks, signs, and prevention explained | Rao Dermatology
- Skin cancer screening: early detection and prevention | Rao Dermatology
- Role of dermatologists in skin cancer: A guide for patients | Rao Dermatology
Filed under: