
Discover what is dermatoscopy and how this advanced technique aids in early skin cancer detection, ensuring your skin health is a priority.

Many dangerous skin cancers look completely ordinary to the naked eye. A mole that seems flat and unremarkable can hide structural warning signs in the deeper layers of your skin that a standard visual check simply cannot reveal. That gap between what you see and what is actually there is exactly where dermatoscopy steps in. As a non-invasive in vivo technique that visualizes subsurface structures in the epidermis, dermoepidermal junction, and superficial dermis, dermatoscopy gives your dermatologist a much sharper picture. This guide walks you through what the technology is, how it works, and why it matters for your long-term skin health.
Table of Contents
- What is dermatoscopy? Basics explained
- How does dermatoscopy work? Devices and techniques
- Dermatoscopy for skin cancer detection: Benefits and accuracy
- Limitations and best practices: What patients should know
- A dermatologist’s take: The real value of dermatoscopy
- Take charge of your skin health with expert help
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Reveals hidden risks | Dermatoscopy lets doctors see skin details missed by the naked eye for earlier detection. |
| Boosts diagnostic accuracy | Studies show dermatoscopy increases reliability in finding melanomas and other skin cancers. |
| Not a replacement for biopsy | A tissue sample may still be needed when results are unclear or for aggressive lesions. |
| Expert skill matters most | Dermatoscopy’s true value depends on the clinician’s training and how findings guide next steps. |
What is dermatoscopy? Basics explained
Standard skin checks rely on reflected light and what the eye can observe on the surface. That approach catches obvious changes, but it leaves a significant amount of diagnostic information hidden beneath the outermost skin layer. Dermatoscopy changes that equation entirely.
Dermatoscopy (also called dermoscopy) is a non-invasive examination method that uses a handheld device called a dermatoscope to look beneath the skin’s surface without cutting or breaking it. Subsurface skin structures in the epidermis, the dermoepidermal junction, and the superficial dermis become visible during this exam. Those layers hold critical information about pigment patterns, vascular structures, and tissue organization that predict whether a lesion is benign or dangerous.
The device accomplishes this by combining three core components: illumination, magnification, and an interface medium. The light source eliminates glare. Magnification, typically between 10x and 100x depending on the device, enlarges fine structural details. The interface medium, often an oil or gel applied to the skin in non-polarized mode, reduces specular reflectance and allows the light to penetrate up to 100 microns beneath the surface.
Here is a quick comparison of what standard visual exams and dermatoscopy each reveal:
| Feature examined | Naked eye exam | Dermatoscopy |
|---|---|---|
| Surface color changes | Yes | Yes |
| Pigment network patterns | No | Yes |
| Vascular structures | No | Yes |
| Milia-like cysts | No | Yes |
| Dermoepidermal junction | No | Yes |
| Subsurface lesion borders | No | Yes |
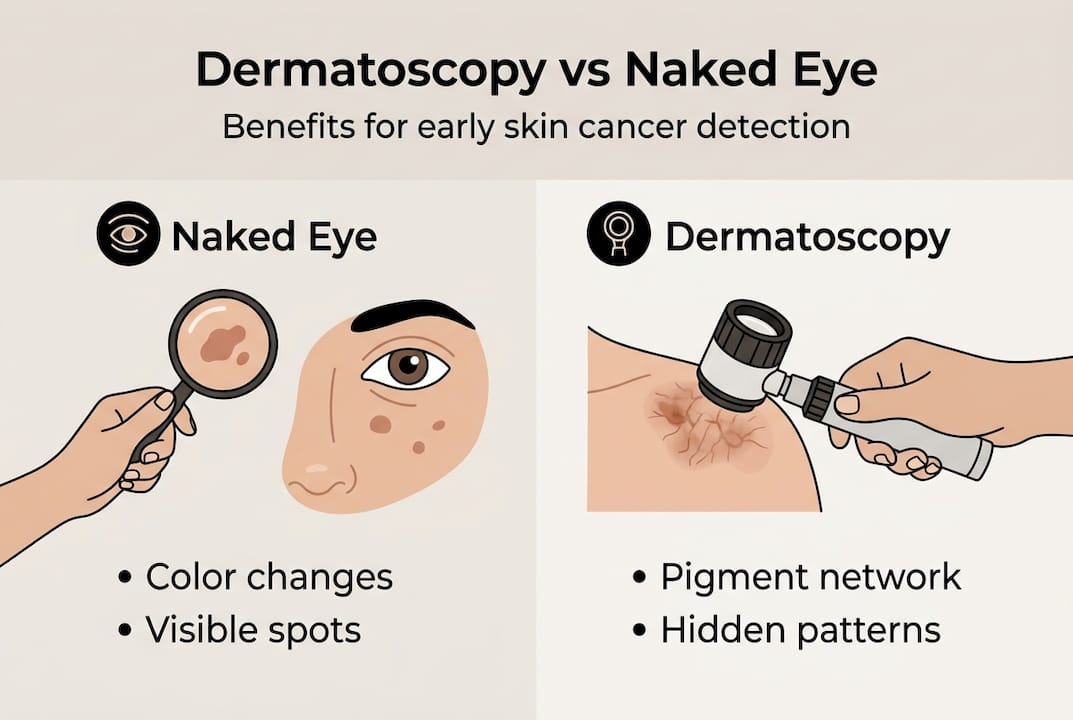
The difference is not subtle. Dermatoscopy can reveal color variations, atypical network patterns, white scar-like areas, and irregular vessel formations that are invisible without magnification and light penetration. These details dramatically change the way a dermatologist categorizes a lesion.
Key things dermatoscopy can identify that standard checks miss:
- Atypical pigment networks in early melanoma
- Blue-white veils and regression structures
- Arborizing vessels typical of basal cell carcinoma (BCC)
- Comma vessels seen in dermal nevi
- Milia-like cysts in seborrheic keratoses
- Dotted vessels common in certain inflammatory conditions
Understanding medical dermatology essentials helps put dermatoscopy in context. It is not a standalone gadget. It is a specialized skill that dermatologists integrate into a complete diagnostic workflow.
Pro Tip: Before your dermatoscopy appointment, avoid applying creams or tanning products to the area being examined. Clean, bare skin gives the dermatoscope its clearest view.

How does dermatoscopy work? Devices and techniques
With the basics in mind, let’s explore how dermatoscopy is performed and the technology behind it.
Not all dermatoscopes work the same way. The two main categories are polarized and non-polarized devices, and the difference between them is clinically meaningful.
Non-polarized dermatoscopes require direct skin contact and need an interface medium like ultrasound gel or mineral oil. This contact reduces the reflection at the skin’s surface and allows light to penetrate the outer layers. The result is a clear view of superficial structures such as scales, milia-like cysts, and the stratum corneum. Non-polarized dermoscopy excels at visualizing features close to the skin surface.
Polarized dermatoscopes use cross-polarization filters that cancel out reflected light without needing any physical contact or interface medium. This allows the light to reach deeper structures like vascular patterns and pigment networks without a gel or oil. The trade-off is that polarized devices show different, deeper structures and can miss some superficial details that non-polarized devices capture beautifully.
The cost difference between these two approaches is real. A polarized unit costs around $324 compared to approximately $35 for a non-polarized device. That gap matters in teledermoscopy settings, where image quality has to carry the full diagnostic load.
| Factor | Polarized dermatoscope | Non-polarized dermatoscope |
|---|---|---|
| Contact required | No | Yes |
| Interface medium needed | No | Yes (oil or gel) |
| Structures visualized | Deep: vessels, pigment | Superficial: scales, cysts |
| Approximate cost | ~$324 | ~$35 |
| Best for | Vascular lesions, deep pigment | Surface texture, milia, scales |
| Use in teledermoscopy | Higher image quality | Lower image quality |
From a patient’s perspective, the actual exam is straightforward. Here is what typically happens during a dermatoscopy examination:
- Preparation: Your dermatologist cleans the area and, if using a non-polarized device, applies a small amount of oil or gel to the skin.
- Device placement: The dermatoscope is gently pressed against or held close to the skin surface.
- Illumination and magnification: The device lights and magnifies the lesion, revealing its internal structure.
- Image capture: Many modern devices connect to digital software, allowing the dermatologist to capture and store images for comparison over time.
- Pattern analysis: The dermatologist evaluates pigment networks, border characteristics, vascular patterns, and color variations using established diagnostic algorithms.
- Clinical decision: Based on findings, the dermatologist recommends monitoring, additional imaging, or biopsy.
Scheduling an annual skin cancer screening that includes dermatoscopy is one of the smartest preventive steps you can take. Serial imaging over time also helps detect subtle changes that might be missed during a single visit.
Dermatoscopy for skin cancer detection: Benefits and accuracy
Understanding the procedure is important, but what really matters is dermatoscopy’s impact on your health, especially skin cancer detection.
Skin cancer is the most commonly diagnosed cancer in the United States, and early detection is the single most reliable factor in improving outcomes. Dermatoscopy significantly raises the probability that your dermatologist will catch a dangerous lesion before it progresses.
“Dermatoscopy improves diagnostic accuracy for melanoma and basal cell carcinoma, achieving sensitivity for BCC between 67.6% and 98.6% with a positive predictive value (PPV) of 85.9% to 97%.”
That range reflects variations in physician experience, device type, and lesion presentation. The upper bounds of those numbers represent expert-level, technology-assisted diagnosis that far outperforms unaided visual examination. For melanoma, AUC reaching 0.802 for metastasis prediction is comparable to histopathology markers like Breslow thickness and ulceration status.
The cancers that benefit most from dermatoscopy include:
- Melanoma: Dermatoscopy detects atypical pigment networks, regression structures, and blue-white veils characteristic of early and advanced melanoma.
- Basal cell carcinoma (BCC): Arborizing vessels, blue-gray ovoid nests, and leaf-like areas are BCC hallmarks visible only through dermatoscopy.
- Squamous cell carcinoma (SCC): Dotted and glomerular vessel patterns, white circles, and keratin structures help distinguish SCC from benign lesions.
- Actinic keratosis: Strawberry pattern and surface scale changes are identifiable pre-cancerous signals.
- Melanocytic nevi: Regular pigment networks and globular patterns confirm benign moles, reducing unnecessary biopsies.
The last point matters more than most patients realize. Dermatoscopy does not just find cancers. It also confidently identifies benign lesions that do not need to be removed. That specificity reduces unnecessary biopsies, spares patients anxiety and recovery time, and lowers overall healthcare costs.
Reading our melanoma guide gives you a strong foundation for understanding what your dermatologist looks for when evaluating suspicious pigmented lesions. Combining that knowledge with regular expert exams is a genuinely proactive strategy. For a full picture of your options, learning more about skin cancer detection and treatment at Rao Dermatology will show you how dermatoscopy fits into a broader care plan.
One practical example of dermatoscopy’s real-world impact: studies show that dermatoscopy-assisted diagnosis reduces unnecessary excisions by up to 42% compared to naked-eye examination alone, while simultaneously increasing the detection rate of true malignancies. That is a better outcome for everyone.
Limitations and best practices: What patients should know
While dermatoscopy is powerful, every test has its boundaries. Here’s what every patient should consider.
Dermatoscopy is not a perfect tool, and knowing where it struggles helps you and your dermatologist use it wisely.
Situations where dermatoscopy performs less reliably include:
- Non-pigmented lesions: Amelanotic melanomas and certain non-pigmented BCCs lack the visual cues that dermatoscopy algorithms rely on, making them harder to classify accurately.
- Skin of color: Lower accuracy in diverse skin tones is an active area of research. Physiologically darker skin can make it harder to distinguish normal pigmentation patterns from abnormal ones.
- Superficial BCC on the trunk or extremities: These lesions can present with subtle features that fall below reliable detection thresholds.
- Certain alopecias: Hair loss conditions examined through dermoscopy of the scalp (trichoscopy) require additional expertise.
- Edge case lesions: Lesions that fall between clear diagnostic categories often require biopsy regardless of dermatoscopy findings.
Physician experience is arguably the most important variable in dermatoscopy outcomes. Expert training boosts diagnostic accuracy by up to 49% compared to untrained observers using the same device. A highly accurate dermatoscope in the hands of an inexperienced examiner produces far less reliable results than a basic device used by an experienced clinician who has evaluated thousands of lesions.
This is why complementary use of both polarized and non-polarized modes is considered best practice. Each mode reveals different structural layers. Using both gives the most complete picture and catches features that either mode alone might miss.
When should a biopsy still happen? Dermatoscopy helps triage lesions, but dermatopathology confirmation through tissue sampling remains the gold standard when any ambiguity exists. Your dermatologist should use dermatoscopy to inform, not replace, histopathological analysis in uncertain cases.
Best practices to maximize dermatoscopy’s value in your care:
- Schedule regular screenings rather than waiting for visible changes
- Ask your dermatologist which mode they use and why
- Request digital imaging so changes can be tracked over time
- Use a skin self-examination guide between appointments to monitor your own skin
- Disclose any new symptoms, itching, or bleeding near a lesion at every visit
Pro Tip: If you have a personal or family history of melanoma, ask your dermatologist about full-body digital dermoscopy mapping. It creates a baseline photographic record that makes subtle changes in lesions easier to detect over time.
A dermatologist’s take: The real value of dermatoscopy
Here is where the conversation shifts from facts to perspective. In over 25 years of evaluating skin lesions, what we have seen time and again is that the technology itself is only as valuable as the clinician interpreting it.
The common misconception is that dermatoscopy is a machine that catches cancer. It is not. It is a visualization tool that shows a trained specialist features they could not otherwise see. The diagnostic leap still happens inside the physician’s mind, drawing on pattern recognition built through thousands of exams. That experience is irreplaceable.
There is also a partnership dimension that patients rarely consider. The best dermatoscopy outcomes happen when patients show up consistently, disclose accurate histories, and stay engaged in monitoring. An annual exam matters. So does the conversation you have when something feels different about a lesion between visits.
We have always emphasized that advanced melanoma detection is not a single-visit event. It is a strategy built over years of observation, repeat imaging, and a solid relationship between patient and specialist. Dermatoscopy significantly aids preventive skin cancer care through non-invasive early detection, but the tool requires ongoing training, careful selection of polarized versus non-polarized modes, and histopathology confirmation when edge cases arise. Technology is the amplifier. Clinical judgment is the signal.
Take charge of your skin health with expert help
If reading this has made you realize that your current skin checks might not be catching everything, you are already thinking the right way. Proactive skin health means getting the right eyes on your skin, with the right tools, on a consistent schedule.
At Rao Dermatology, our board-certified dermatologists bring over 25 years of specialized experience to every skin exam, including advanced dermatoscopy-assisted evaluations across our California, New Jersey, and New York locations. We combine expert clinical judgment with digital imaging technology to give you the most accurate, personalized assessment possible. From your first screening to any necessary follow-up, our skin cancer screening and care services and dermatopathology services are designed to keep you ahead of risk, not reacting to it.
Frequently asked questions
Is dermatoscopy painful or invasive?
Dermatoscopy is completely non-invasive and painless, using a handheld device gently placed on the skin surface with no cutting, needles, or discomfort involved.
Can dermatoscopy detect all types of skin cancer?
Dermatoscopy is highly effective for pigmented cancers like melanoma and BCC, but lower accuracy for non-pigmented and amelanotic lesions means it works best as part of a complete diagnostic approach.
Is dermatoscopy always accurate?
Dermatoscopy significantly improves diagnostic accuracy over naked-eye exams, but it does not replace biopsy. Histopathology confirmation remains essential when findings are ambiguous or a lesion falls into an edge case category.
What should I do if I find a suspicious spot between exams?
Do not try to diagnose it yourself. Note any changes in size, color, or texture, and contact your dermatologist promptly to schedule an evaluation before your next scheduled screening.
Recommended
- Annual Skin Cancer Screening: Your Complete Guide to Dermatology Checkups | Rao Dermatology
- Complete Guide to At-Home Skin Cancer Checks: What You Need to Know | Rao Dermatology
- Melanoma: A Complete Guide to Skin Cancer Detection, Prevention & Treatment | Rao Dermatology
- Essential Guide to Skin Self-Examination: What to Look for Between Dermatology Visits | Rao Dermatology
Filed under: