
Discover the types of eczema, their symptoms, causes, and effective treatments. Find the relief you need today!

Eczema is defined as a group of inflammatory skin disorders marked by itchiness, dryness, redness, and rash, with each of the major types of eczema requiring its own specific approach to care. The most common form, atopic dermatitis, begins in the first year of life in 60% of cases. Other distinct forms include contact dermatitis, dyshidrotic eczema, nummular eczema, seborrheic dermatitis, and asteatotic dermatitis. Knowing which type you have is the first step toward getting relief that actually works. This guide covers each form’s symptoms, causes, diagnosis, and the latest treatment options available in 2026.
What are the main types of eczema?
Eczema is an umbrella term, not a single disease. Each subtype has a distinct appearance, location on the body, and set of triggers. Recognizing these differences helps you and your dermatologist choose the right treatment path.
Atopic dermatitis
Atopic dermatitis is the most common chronic inflammatory skin disease. It begins in infancy for the majority of patients, and about 60% of childhood cases resolve by age 12. The condition causes intense itching, skin thickening (called lichenification), and redness. It is closely linked to other immune conditions: atopic dermatitis connects with asthma, allergic rhinitis, and food allergies through shared IgE-mediated immune pathways. For a deeper look at this specific form, Raodermatology’s atopic dermatitis guide covers symptoms and treatment in detail.

Contact dermatitis
Contact dermatitis splits into two types: allergic and irritant. Allergic contact dermatitis occurs when the immune system reacts to a specific substance, such as nickel, latex, or fragrance. Irritant contact dermatitis results from direct skin damage caused by chemicals, soaps, or repeated hand washing. Both produce a localized rash that appears where the skin touched the offending substance. The rash typically clears once the trigger is removed.
Dyshidrotic eczema
Dyshidrotic eczema produces small, intensely itchy blisters on the palms, fingers, and soles of the feet. It accounts for 5%–20% of all hand eczema cases. Each flare typically lasts 2–3 weeks before the blisters dry and peel. Triggers include stress, sweating, and exposure to metals like cobalt or nickel. Recurrent episodes are common, making long-term management necessary.
Nummular eczema
Nummular eczema appears as round, coin-shaped plaques on the skin. These patches are often crusted, oozing, or scaly, and they can be mistaken for ringworm or psoriasis. The condition tends to affect the legs, arms, and torso. Dry skin and cold weather are common contributors. Understanding the difference between eczema and psoriasis is useful here, since the two conditions share visual similarities but require different treatments.
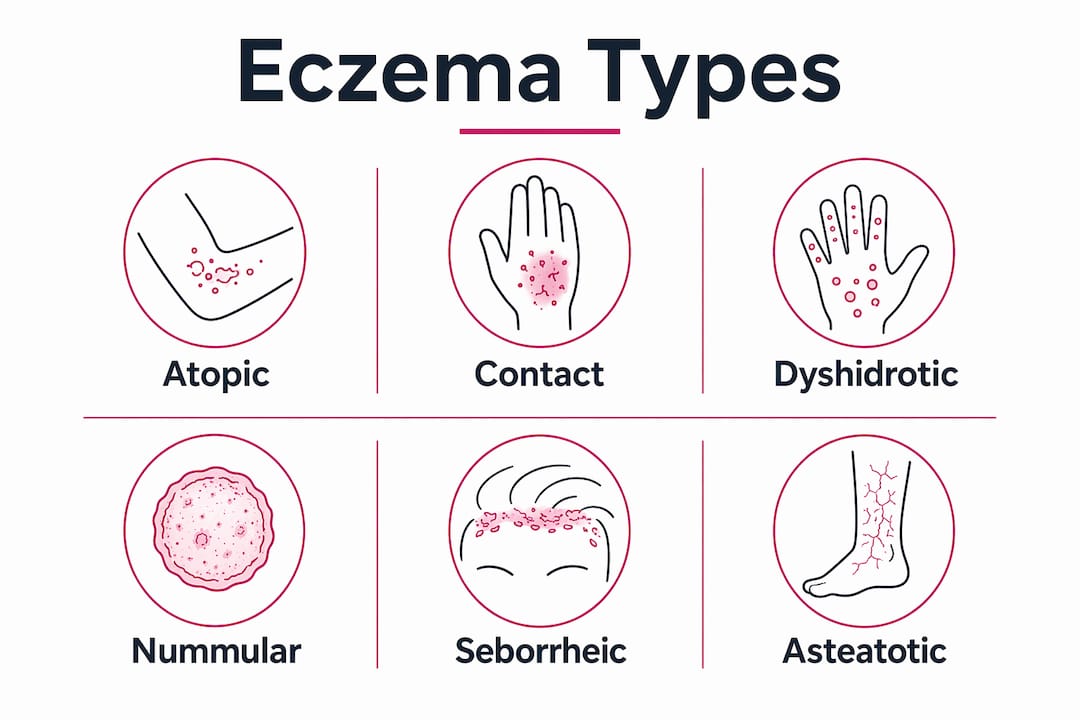
Seborrheic dermatitis
Seborrheic dermatitis targets oil-rich areas of the skin, particularly the scalp, face, and chest. It produces greasy, yellowish scales and redness. In infants, it appears as cradle cap. In adults, it often presents as dandruff or facial flaking around the nose and eyebrows. A yeast called Malassezia plays a role in triggering the inflammatory response in this form.
Asteatotic dermatitis
Asteatotic dermatitis is a form most common in older adults. It affects around 70% of individuals over 60. The skin becomes extremely dry, rough, and cracked due to age-related loss of epidermal lipids. It often looks like a dried riverbed, with a pattern called “eczema craquelé.” The legs are the most frequently affected area.
| Type | Primary location | Key feature |
|---|---|---|
| Atopic dermatitis | Creases, face, hands | Chronic itch, lichenification |
| Contact dermatitis | Site of exposure | Localized rash from allergen or irritant |
| Dyshidrotic eczema | Palms, fingers, soles | Small itchy blisters |
| Nummular eczema | Legs, arms, torso | Coin-shaped plaques |
| Seborrheic dermatitis | Scalp, face, chest | Oily, yellowish scales |
| Asteatotic dermatitis | Lower legs | Cracked, dry skin in older adults |
What causes eczema and what triggers flare-ups?
The causes of different forms of dermatitis vary, but most involve a combination of genetic susceptibility, immune system activity, and environmental exposure. Atopic dermatitis has the strongest genetic component, with mutations in the filaggrin gene weakening the skin barrier and allowing allergens and irritants to penetrate more easily. This barrier dysfunction activates an IgE-driven immune response, producing the characteristic inflammation and itch.
Environmental factors drive flare-ups across nearly all eczema types. Soaps, detergents, fragrances, and stress are among the most common triggers. That means a single load of laundry done with a scented detergent can set off a week-long flare in a sensitive person. Contact dermatitis is entirely trigger-dependent: allergic contact dermatitis requires prior sensitization to a substance, while irritant contact dermatitis can affect anyone exposed to a strong enough chemical. Age plays a direct role in asteatotic dermatitis, where declining oil production in aging skin creates the conditions for chronic dryness and cracking.
Pro Tip: Keep a simple trigger diary for two weeks. Note what you ate, what products touched your skin, your stress level, and the weather. Patterns often emerge faster than you expect.
How is eczema diagnosed?
Diagnosing eczema correctly requires more than looking at a rash. Clinical diagnosis involves assessing rash appearance, distribution, patient history, and itch intensity. No single lab test confirms eczema, which is why the clinical picture matters so much.
Age-specific patterns are a key diagnostic tool. Infants typically develop eczema on the cheeks and scalp, while older children and adults show rashes in skin creases, on the hands, and around the neck. A dermatologist uses these patterns to narrow down the type before any testing begins.
For suspected contact dermatitis, the diagnostic process includes:
- A detailed exposure history covering occupational and household products.
- Skin prick testing to identify IgE-mediated allergic reactions.
- Patch testing, which applies small amounts of common allergens to the back for 48–72 hours to detect delayed allergic reactions.
- Ruling out conditions like psoriasis, tinea (fungal infection), and seborrheic dermatitis that can mimic eczema.
- Referral to a board-certified dermatologist when the diagnosis remains unclear or symptoms are severe.
Getting the right diagnosis matters because treating nummular eczema with an antifungal cream, for example, will not work. The treatment must match the type.
What treatment options exist for different eczema types?
Eczema treatment options range from basic moisturization to advanced biologic therapies, depending on the type and severity of the condition. The foundation of care for every eczema subtype is consistent skin hydration. Emollients and moisturizers repair the skin barrier and reduce the frequency of flares when used correctly.
The most effective treatments by category include:
- Moisturizers and emollients: Apply thick creams or ointments immediately after bathing. Applying moisturizer within three minutes of leaving the bath locks in moisture before the skin dries. This single habit reduces flare frequency significantly.
- Topical corticosteroids: The standard prescription treatment for active flares. Strength is matched to the body area and severity. Overuse causes skin thinning, so short-term use under medical guidance is the correct approach.
- Non-steroidal topical agents: Calcineurin inhibitors like tacrolimus and pimecrolimus work on sensitive areas such as the face and eyelids where steroids carry higher risk.
- JAK inhibitors and monoclonal antibodies: The 2026 American Academy of Dermatology guidelines introduce targeted therapies including monoclonal antibodies and JAK inhibitors for moderate-to-severe atopic dermatitis. These therapies block specific immune pathways driving inflammation rather than suppressing the immune system broadly.
- Phototherapy: Narrowband UVB light therapy is used for widespread or treatment-resistant eczema. It reduces inflammation and itch without the systemic side effects of oral medications.
- Systemic immunosuppressants: Cyclosporine and methotrexate remain options for severe cases that do not respond to other treatments.
Pro Tip: For seborrheic dermatitis specifically, medicated shampoos containing ketoconazole or selenium sulfide used twice weekly can control scalp flares more effectively than topical steroids alone.
The expanding range of targeted biologic therapies marks a real shift beyond traditional corticosteroids. Patients who spent years cycling through ineffective treatments now have options that address the root immune dysfunction.
How to manage eczema daily and prevent flare-ups
Daily management is where most eczema control actually happens. Prescription medications treat active flares, but consistent habits prevent them. The itch-scratch cycle is the biggest obstacle: scratching damages the skin barrier, which increases inflammation, which intensifies the itch. Breaking this cycle is as important as any medication.
Practical daily habits that reduce flare frequency:
- Bathe in lukewarm water for no more than 10 minutes. Hot water strips natural oils and worsens dryness.
- Apply a fragrance-free, thick moisturizer within three minutes of bathing, every single day.
- Wear soft, breathable fabrics like cotton. Avoid wool and synthetic materials directly against the skin.
- Use fragrance-free, dye-free laundry detergent and avoid fabric softeners.
- Keep fingernails short to minimize skin damage from nighttime scratching.
- Manage stress through regular physical activity, sleep, and relaxation techniques, since stress is a documented flare trigger.
Knowing when to seek professional care is part of managing eczema well. If your skin becomes infected (signs include warmth, crusting, and pus), if over-the-counter treatments stop working, or if eczema is affecting your sleep and daily life, a dermatologist visit is the right next step. Raodermatology’s eczema management tips offer additional guidance from experienced NYC dermatologists.
Key Takeaways
Identifying the correct type of eczema is the single most important step toward effective treatment, since each subtype has distinct triggers, symptoms, and therapies.
| Point | Details |
|---|---|
| Eczema is not one disease | Six distinct types exist, each with unique symptoms, locations, and causes. |
| Atopic dermatitis is most common | It starts in infancy for 60% of patients and links to asthma and allergies. |
| Triggers drive most flares | Soaps, fragrances, stress, and weather are the most common and avoidable culprits. |
| Moisturize within three minutes | Applying emollients immediately post-bath is the most effective barrier-repair habit. |
| New therapies change outcomes | JAK inhibitors and monoclonal antibodies now offer targeted relief for moderate-to-severe cases. |
Why eczema care is more personal than most people realize
Eczema is one of those conditions where the standard advice, “moisturize and avoid triggers,” is technically correct but practically incomplete. What I see consistently is that patients arrive having tried every drugstore cream available, frustrated that nothing works. The problem is rarely the product. The problem is that they are treating the wrong type.
Nummular eczema does not respond the same way atopic dermatitis does. Seborrheic dermatitis on the face needs a completely different approach than dyshidrotic eczema on the hands. Applying the same routine across all of them is like using the same key for every lock. The chronic itch compounds the frustration because it disrupts sleep, concentration, and confidence in ways that are hard to explain to someone who has not experienced it.
The shift toward targeted biologics and JAK inhibitors is genuinely exciting from a clinical standpoint. For years, moderate-to-severe atopic dermatitis had limited options beyond cyclosporine, which carries real systemic risks. Now patients have therapies that address the specific immune pathways causing their inflammation. The catch is that these treatments require accurate diagnosis and specialist oversight to use safely and effectively.
Patient education remains the most underrated part of eczema management. Understanding the itch-scratch cycle, knowing your personal triggers, and applying moisturizer correctly sounds basic. In practice, these habits determine whether a patient stays in remission or cycles through flares every few weeks. The medication gets the credit, but the daily routine does the real work.
— Krunal
Raodermatology’s approach to eczema diagnosis and care
Living with persistent skin irritation, recurring rashes, or uncontrolled itching deserves more than a generic treatment plan.
Raodermatology’s medical dermatology services cover the full spectrum of eczema care, from accurate type-specific diagnosis to access to the latest targeted therapies. With 25+ years of experience across New Jersey, New York, and California, the practice builds personalized care plans based on your skin’s specific needs. Whether you are dealing with a first flare or a condition that has not responded to previous treatment, a board-certified dermatologist can give you a clear diagnosis and a path forward. Schedule a consultation to get answers that actually match your symptoms.
FAQ
What is the most common type of eczema?
Atopic dermatitis is the most common type, beginning in the first year of life in 60% of cases. It is a chronic inflammatory condition closely linked to asthma and allergic rhinitis.
How do I know if I have contact dermatitis or atopic dermatitis?
Contact dermatitis appears in a localized area where skin touched a specific allergen or irritant, while atopic dermatitis typically follows a chronic, widespread pattern in skin creases. Patch testing performed by a dermatologist confirms contact dermatitis.
Can eczema be cured permanently?
There is no permanent cure for most eczema types, but many patients achieve long-term remission through consistent skin care, trigger avoidance, and appropriate medical treatment. About 60% of childhood atopic dermatitis cases resolve by age 12.
What triggers eczema flare-ups?
Soaps, detergents, fragrances, stress, and weather changes are the most common flare triggers across eczema types. Identifying your personal triggers through a diary is the most reliable way to reduce flare frequency.
Are new eczema treatments available in 2026?
The 2026 American Academy of Dermatology guidelines introduce monoclonal antibodies and JAK inhibitors for moderate-to-severe atopic dermatitis. These targeted therapies address specific immune pathways and offer meaningful relief for patients who have not responded to traditional treatments.
Recommended
- Eczema: Complete Guide to Symptoms, Types, Causes, and Treatment Options | Rao Dermatology
- Effective Eczema Treatment and Management: Expert Tips from NYC Dermatologists | Rao Dermatology
- What Is Eczema? Complete Guide to Causes, Symptoms & Effective Treatment Options | Rao Dermatology
- Psoriasis vs Eczema: Key Differences in Symptoms, Causes & Treatment Options | Rao Dermatology
Filed under: